
By Boyd Tomasetti, D.M.D., Malachi Zeitner, D.D.S., Ayrton Sanguino, D.M.D., Sara Anderson, D.D.S., M.D. From the Winter 2026 Journal of the Colorado Dental Association
Medication-Related Osteonecrosis of the Jaw (MRONJ) is a rare and serious condition that occurs in patients taking medications prescribed for the treatment of cancer and osteoporosis. It is characterized by necrosis of mandibular or maxillary bone following exposure to antiresorptive and antiangiogenic agents. MRONJ is particularly prevalent in patients who have taken bisphosphonates (e.g., alendronate or zoledronic acid) or RANKL inhibitors (e.g., denosumab). MRONJ can occur spontaneously in the setting of acute or chronic infection as well as after a dental procedure, such as a tooth extraction.
Antiresorptive medications have a direct effect on osteoclast formation and function. Multiple clinical studies have confirmed that dysfunctional osteoclasts have an impact on MRONJ pathophysiology by suppressing bone remodeling. Poor oral hygiene coupled with periodontal disease and periapical pathology contribute to MRONJ development.
The diagnosis of MRONJ requires three separate elements: 1) exposed bone or bone that can be probed through an intraoral or extraoral fistula in the maxillofacial region that does not heal within eight weeks, 2) a patient with a history of antiresorptive or antiangiogenic therapy and 3) no history of radiation therapy or metastatic disease to the jaws. Other signs and symptoms can include pain, swelling, infection, loose teeth and intraoral/extraoral drainage. In advanced stages, the condition can lead to extensive bone loss, pathologic fractures and chronic infection. A definitive MRONJ diagnosis is based on patient history, physical examination and imaging. Imaging, including panoramic radiographs and cone-beam CT scans, can help assess the extent of bone involvement, although findings can be non-specific in early stages. There are no laboratory tests that are diagnostic of MRONJ. Multiple studies have concluded that serum CTX levels, previously considered biomarkers, are not reliable predictors for MRONJ.[i] [ii]
The American Association of Oral and Maxillofacial Surgeons (AAOMS) classifies MRONJ into four stages.1 Management strategies will depend on the stage and may range from conservative treatment, including antimicrobial mouth rinses and systemic antibiotics, to surgical debridement or resection in severe cases. AAOMS recommends that because 50% of Stage 0 progress to Stage 1, it should be considered a precursor to MRONJ.
Medications associated with MRONJ fall into a few categories: bisphosphonates, RANKL inhibitors, and other monoclonal antibodies. Bisphosphonates are antiresorptive medications used in cancer therapy and osteoporosis treatment. They are given both orally [e.g., alendronate (Fosamax) and risedronate (Actonel)] and parenterally [e.g., zoledronic acid (Zometa and Reclast) and ibandronate (Boniva)]. RANKL inhibitors, like denosumab (Prolia and Xgeva), are antiresorptive agents that inhibit osteoclast function. Other monoclonal antibody medications that are not RANKL inhibitors, such as romosozumab (Evenity), are also used in osteoporosis treatment. An increased MRONJ risk has been found in patients taking both corticosteroids and antiresorptive medications.
MRONJ Risk Factors
As practitioners, it is important that we understand the risk of performing dental procedures on our patients and that we inform patients of the risk of developing MRONJ as a sequela to the proposed treatment. The literature is quite specific in stating that the risk of MRONJ is considerably higher in patients being treated for a malignancy than in patients being treated for osteoporosis.[iii] [iv] The risk of MRONJ in cancer patients exposed to bisphosphonates is 2-10 times higher than those with no exposure. Recent clinical trials show that the overall risk in cancer patients is less than 5%.1
The risk of developing MRONJ in patients taking osteoporotic medications is considerably less than in cancer patients. The MRONJ risk in those patients taking bisphosphonates is 0.02% to 0.05%. Those taking oral medications have a higher risk — five per 10,000 versus two per 10,000. Patients taking RANKL inhibitors have a much higher incidence of developing MRONJ — 0.3%. Romosozumab has had minimal research with respect to MRONJ but appears to be in the 0.03% to 0.05% range, similar to bisphosphonates. The duration of antiresorptive therapy plays an important role as a risk factor in both cancer and osteoporosis patients. Recent studies have suggested that there is a significant increase in MRONJ in cancer patients after 24 months of both bisphosphonate and RANKL inhibitors.[v] [vi] In osteoporosis patients, there have been mixed reports with some showing a marked increase after four years of therapy.
Conclusion
MRONJ poses significant challenges particularly given the widespread use of bisphosphonates and denosumab in older and cancer-affected populations. Communication between oncologists, primary care physicians and dental professionals is essential for the prevention and management of MRONJ.
Preventive dental care plays a crucial role in reducing MRONJ risk.[vii] Patients scheduled to begin antiresorptive therapy should ideally undergo a dental examination and complete any necessary invasive dental procedures beforehand. Good oral hygiene, regular dental visits and avoidance of invasive dental work are essential. When extractions or surgery are necessary, conservative techniques and prophylactic antibiotics may reduce the risk of complications. Extraction of carious or periodontally hopeless teeth should not be delayed if indicated. It is imperative that time be given for good soft tissue healing and bone coverage after extractions.
Ongoing research is exploring new therapeutic strategies for MRONJ, including the use of platelet-rich plasma (PRP), teriparatide (a parathyroid hormone analog that stimulates bone formation), and low-level laser therapy. However, results have been variable, and at this time there is no universally accepted treatment for advanced MRONJ.
In summary, MRONJ is a serious but often preventable complication of antiresorptive and antiangiogenic medications. Awareness of risk factors, early diagnosis, preventive care, and a patient-specific treatment approach can help minimize morbidity and improve outcomes in affected patients. If possible, any invasive dental procedures should be done prior to starting any of these medications.
Case 1
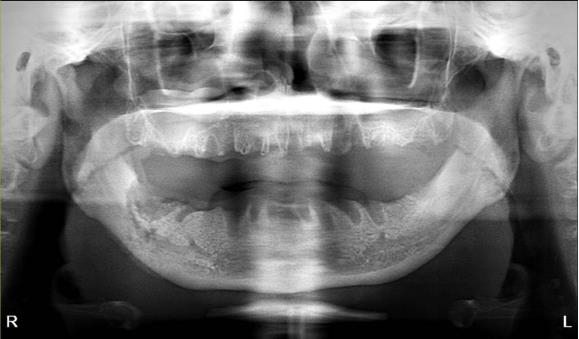
The patient is an 80-year-old female with a history of osteoporosis for which she received Alendronate (Fosamax) 70 mg one time per week for 12 years. She stopped the medication in December 2023. She was initially seen at Denver Health in January 2024 with concerns of pain and swelling on the lower right side that had persisted for over 10 months. Her dentist had removed tooth #28 and placed an osseo-integrated implant in 2020.
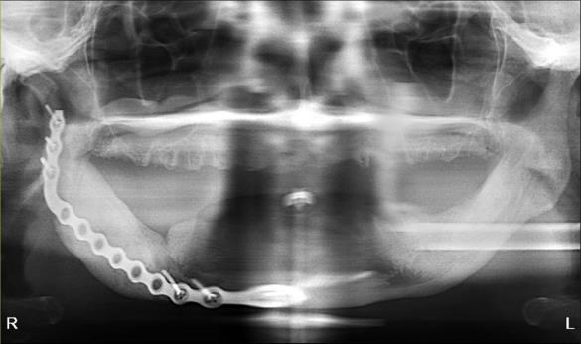
The patient was noted to have extensive erosive bony changes in the right mandibular body. She was diagnosed with Stage 3 MRONJ. The mandible was resected through a submandibular approach and a reconstruction bar was placed. She is now doing well without recurrence of her MRONJ and has elected not to have definitive bony reconstruction.
 |
 |
 |
 |
Case 2
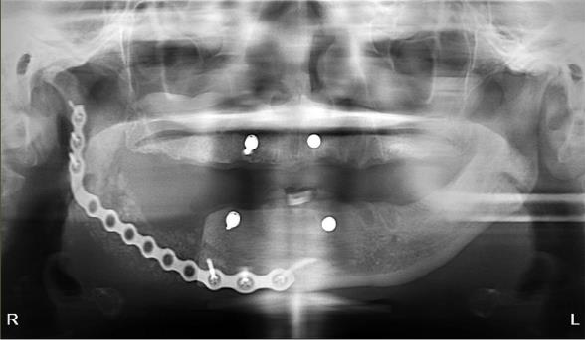
The patient is a 54-year-old female with a history of Stage 4 metastatic breast cancer treated with chemotherapy and radiation. She was treated with zoledronic acid (Zometa) beginning in June 2020. The patient was referred to Denver Health OMS by her dentist regarding non-healing extraction sites and additional extractions. In mid-2022, about three months prior to the referral, her dentist had extracted teeth #29 to #31. On examination, the patient had Stage 2 MRONJ along with painful, periodontally compromised, non-restorable teeth. Following a consultation with oncology and infectious disease, the decision was made to debride the MRONJ area and remove the remaining teeth in the operating room with the patient on long-term antibiotic coverage. Within two to three months, MRONJ had recurred and in April 2023, the patient subsequently underwent a right posterior mandibular resection with an antibiotic spacer placed in the resected area.
 |
 |
 |
 |
Case 3
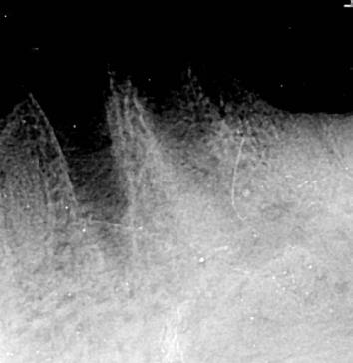
The patient is a 76-year-old female with a history of multiple myeloma who was referred by her dentist for a full mouth extraction prior to starting Zolendronic acid (Zometa) infusions. Her past medical history was further complicated by cardiovascular and pulmonary issues, along with Type II diabetes and general frailty. After discussion with her dentist, the decision was made to switch from full mouth extractions to removal of symptomatic teeth. The patient underwent removal of teeth #20, #23, #24 and #27 in August 2023 and began her infusions three months later. The patient did well and returned for removal of teeth #21 and #22 in the spring of 2025. At that time, she had also been started on a combination of daratumumab (Darzalex), a monoclonal antibody, and bortezomib (Velacade), a proteasome inhibitor, for her multiple myeloma. After two months, the patient developed pain and bone exposure at the site of #21/#22. She also reported pain in teeth #5, #14 and #16. She was diagnosed with Stage 2 MRONJ. The area was debrided and teeth #5, #14 and #16 were removed. Currently, she is pain-free and there is no evidence of bone exposure or MRONJ.
 |
 |
 |
 |
Dr. Boyd Tomasetti is an attending surgeon at Denver Health OMS Residency program. He is a past president of the American Association of Oral and Maxillofacial Surgeons and the Colorado Society of Oral and Maxillofacial Surgeons. He is Board Certified by the ABOMS.
Dr. Malachi Zeitner is a graduate of the University of Iowa School of dentistry and is a third-year resident in the Denver Health OMS Residency program.
Dr. Ayrton Sanguino is a graduate of Rosemont School of Dental Medicine and is a first-year resident at Denver Health OMS Residency program.
Dr. Sara Anderson is the Chief of Oral and Maxillofacial Surgery and OMS Residency Program Director at Denver Health. She is a Board-Certified OMS and one of the cofounders of The Women in Oral and Maxillofacial Surgery Symposium.
[1] AAOMS White Paper Medication Related Osteonecrosis of the Jaw 2022. [1] Salgueiro M, Stribos M, Zhang LF, Stevens M, Awad ME, Elsalanty M. Value of pre-operative CTX serum levels in the prediction of medication-related osteonecrosis of the jaw (MRONJ): a retrospective clinical study. EPMA Journal. 2019 January 24;10(1):21-29. [1] Yarom N, Shapiro CL, Peterson DE, Van Poznak CH, Bohlke K, Ruggiero SL, Migliorati CA, Khan A, Morrison A, Anderson H, Murphy BA, Alston-Johnson D, Mendes RA, Beadle BM, Jensen SB, Saunders DP. Medication-Related Osteonecrosis of the Jaw: MASCC/ISOO/ASCO Clinical Practice Guideline. Journal of Clinical Oncology. 2019 September 1;37(25):2270-2290. [1] El-Ma’aita A, Da’as N, Al-Hattab M, Hassona Y, Al-Rabab’ah M, Al-Kayed MA. Awareness of the risk of developing medication-related osteonecrosis of the jaw among bisphosphonate users. J Int Med Res. 2020 Sep;48(9):300060520955066. [1] Ghidini G, Manfredi M, Giovannacci I, Mergoni G, Sarraj A, Mureddu M, Giunta G, Bonanini M, Meleti M, Vescovi P. Medication-related osteonecrosis of the jaw: risk factors in patients under biphosphonate versus patients under antiresorptive-antiangiogenic drugs. Minerva Stomatologica. 2017 August;66(4):135-140. [1] Yarom N, Shapiro CL, Peterson DE, Van Poznak CH, Bohlke K, Ruggiero SL, Migliorati CA, Khan A, Morrison A, Anderson H, Murphy BA, Alston-Johnson D, Mendes RA, Beadle BM, Jensen SB, Saunders DP. Medication-Related Osteonecrosis of the Jaw: MASCC/ISOO/ASCO Clinical Practice Guideline. Journal of Clinical Oncology. 2019 September 1;37(25):2270-2290. [1] Alblazi K, Nabil S, Tumian NR, Yunus SSM, Ramli R. Potential role of comprehensive dental care in preventing medication related osteonecrosis of the jaw (MRONJ): a single centre study. BMC Oral Health. 2024 October 26;24(1):1291.