
Authors: Chaitanya Puranik, B.D.S., M.S., MDentSci, Ph.D.1; Shahbaz Katebzadeh, D.M.S., M.S.2; Paloma Reyes-Nguyen, D.M.D, M.S.D.3; Katherine Chin, D.D.S., M.S.4; Catherine Flaitz, D.D.S., M.S..5
Authors Affiliations:1Associate Professor and Residency Program Director, Department of Pediatric Dentistry, Children’s Hospital Colorado and School of Dental Medicine, University of Colorado.
2Assistant Professor, Department of Pediatric Dentistry, Children’s Hospital Colorado and School of Dental Medicine, University of Colorado.
3Assistant Professor and Director of Predoctoral Dental Education, Department of Pediatric Dentistry, Children’s Hospital Colorado and School of Dental Medicine, University of Colorado.
4Associate Professor, Chief Medical Director, and Chair, Department of Pediatric Dentistry, Children’s Hospital Colorado and School of Dental Medicine, University of Colorado.
5Professor and Chair, Department of Diagnostic Sciences, School of Dental Medicine, University of Colorado.
Corresponding Author: Chaitanya Puranik, B.D.S., M.S., MDentSci, Ph.D., Associate Professor and Residency Program Director, Department of Pediatric Dentistry, Children’s Hospital Colorado and School of Dental Medicine, University of Colorado;
chaitanya.puranik@childrenscolorado.org, 720-777-2719.
Conflicts of interest: The authors declare no conflicts of interest.
Keywords: Cemental tear, dental trauma, pediatric dentistry, root fracture, conservative management
Abstract
Cemental tear (CT) is an underrecognized condition in pediatric dentistry, often misdiagnosed due to its radiographic similarity to other periodontal and endodontic pathologies. This report describes a rare case of CT in a 10-year-old girl following traumatic dental injury, involving both a detached cemental fragment on maxillary right central incisor with an associated apical-middle third root fracture, and an undetached cemental tear on maxillary left central incisor. The patient was managed conservatively with no immediate treatment and monitored periodically over two years. Radiographs revealed spontaneous resolution of the detached CT and stabilization of the root fracture, with both teeth remaining asymptomatic and vital during the two-year follow-up period. This case highlights the potential for spontaneous healing in pediatric CT cases, emphasizing the importance of conservative management and close monitoring in the absence of symptoms. Increased awareness among general and pediatric dental practitioners may prevent unnecessary interventions and promote preservation of natural teeth in children with CT secondary to traumatic dental injuries.
Introduction
Cemental tear (CT) is an underrecognized condition characterized by the partial or complete detachment of cementum from the root surface.1 Often misdiagnosed as vertical root fractures or chronic periodontal-endodontic lesions, CTs are more commonly reported in older adults with predisposing factors such as occlusal trauma, periodontal disease, or bruxism.1–4 The radiographic and clinical presentation of CT overlaps with other dental pathologies, which contributes to under-recognition, especially in pediatric populations.5,6 While CT has been well described in adults, literature on its occurrence and management in children is scarce. Traumatic dental injuries (TDIs), which affect approximately one in three children, may serve as an etiological factor for CT in younger patients.7 This report presents a pediatric case with both detached and undetached CTs and an associated root fracture, with a two-year follow-up, highlighting spontaneous healing and reinforcing the importance of conservative management strategies in similar scenarios. Figure 1A and 1B shows a line drawing of a detached or undetached CT, respectively.
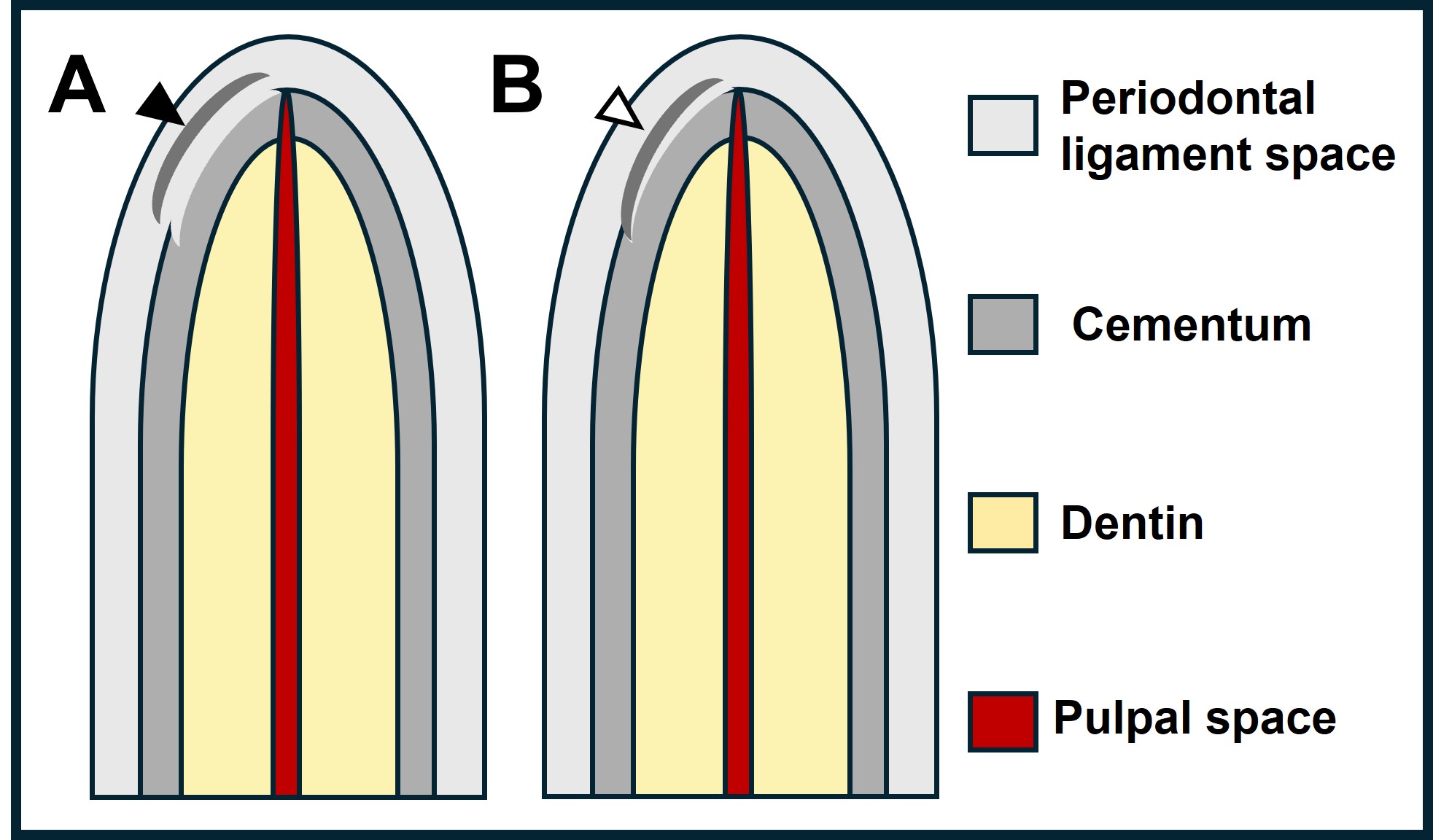
Figure 1: Illustration of a root apex with detached cemental tear (A, black arrow) and undetached or partially detached cemental tear (B, white arrow) fragment.
Case Report
A 10-year-old, African American female presented to the dental clinic at Children’s Hospital Colorado for a routine dental appointment. She had no significant medical or surgical history with no reported allergies to food or medications. The patient’s height, weight and body mass index were 75th percentile for her age. The patient reported a history of TDI to the front teeth due to a fall, three weeks before the dental visit. She reported minor bleeding with no mobility of teeth. Clinical examination was consistent with subluxation of maxillary central incisors. Radiographic assessment of maxillary right central incisor showed a horizontal root fracture at the junction of the apical and middle thirds, accompanied by a vertical linear radiopacity suggestive of a detached CT on the mesial aspect of the root. Maxillary left central incisor demonstrated an undetached CT along the mesial aspect of the apical-root surface without any evident root fracture (Figure 2A and B). Both central incisors were clinically asymptomatic, and cold testing elicited a normal response with both teeth. The clinical and radiographic features led to a diagnosis of CT and root fracture secondary to a TDI. As the reporting was done three weeks after TDI with no obvious clinical signs of mobility or bleeding, no treatment was provided.
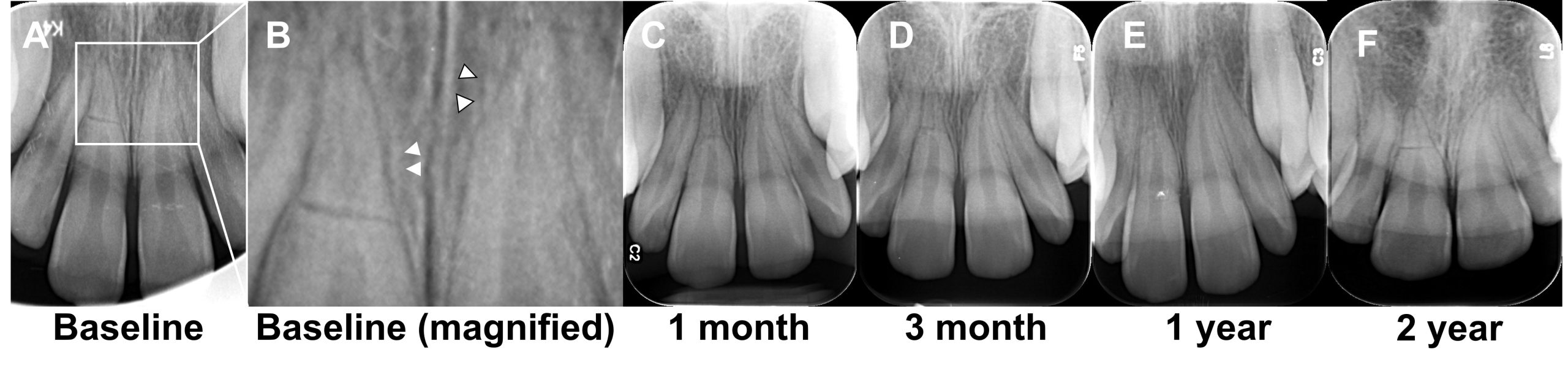
Figure 2: Periapical radiograph of maxillary central incisors three weeks after traumatic dental injury (A). Magnified view of the radiograph at baseline with detached cemental tear (black arrow) and undetached cemental tear (white arrow) on maxillary right and left central incisors, respectively (B). Periapical radiographs at one-month (C), three-month (D), one-year, and two-year (F) follow-up visits.
The patient was placed on a periodic recall schedule with regular clinical and radiographic evaluations as per the International Association of Dental Traumatology recommendations. Post-TDI radiographs at one month, three months, one year, and two years are provided in figures (2C-F), respectively. Over the next two years, both maxillary central incisors remained asymptomatic and functional. Radiographic imaging confirmed widening of the periodontal ligament space near the CT site and later resolution of the CT and stabilization of the root fracture. No endodontic intervention was required.
Discussion
CT is a rare but significant entity, especially in pediatric patients, where the condition is often overlooked. In adults, CT is typically linked to chronic occlusal forces and periodontal compromise.1,2,4 However, in children, low-grade, acute shear forces from TDI are likely contributors to CT, as seen in this case. Detached cemental fragments act as foreign body or foci for bacterial colonization, potentially leading to localized periodontal destruction if not recognized early.3,6
Radiographically, CTs often present as thin, linear radiopaque fragments adjacent to the root surface within the periodontal ligament space. If infection or inflammation is present, the CT fragment could be surrounded by a radiolucency. In case of TDI, multiple periapical radiographs are instrumental in identifying the cemental fragments, as the presence of a vertical root fracture can complicate CT diagnosis due to similar radiographic appearances.9 Although a three-dimensional radiograph may be valuable for diagnosis of CT, it may be impractical in children when the magnitude of trauma is less severe.
Lin et al. reported that CTs most frequently occur in the middle third of the root and are often misdiagnosed, resulting in unnecessary or aggressive periodontal or surgical interventions.9 This case supports a more conservative approach, especially when CT is evident in the apical root areas. Pediatric patients exhibit a higher regenerative capacity, and in asymptomatic teeth with stable periodontal conditions, a non-surgical approach can be effective.10
In a systematic review, Lee et al. proposed a classification system for CT and recommended tailored treatment strategies based on location and symptoms.8 Conservative therapy, including observation and basic periodontal maintenance, is appropriate in cases without significant mobility or infection.10 As demonstrated here, both CT and root fractures in the apical root area may resolve or stabilize over time, particularly when CT is secondary to TDI with vital pulp.
This report adds to the limited pediatric literature and illustrates that detached or undetached CTs resulting from TDI can be successfully managed without surgical, periodontal or endodontic interventions. A conservative approach helps preserve tooth vitality and structural integrity while minimizing patient morbidity.
Key Points: Why this paper is important to general and pediatric dentists
- CTs may occur in children or adults following TDI and can mimic vertical root fractures; careful radiographic analysis is key.
- Conservative management and long-term monitoring may be effective for asymptomatic CTs and root fractures, especially in the apical root area.
- Awareness of CT as a potential post-TDI sequela can help prevent overtreatment and preserve natural dentition.
References
- Haney JM, Leknes KN, Lie T, Selvig KA, Wikesjö UM. Cemental tear related to rapid periodontal breakdown: a case report. J Periodontol. 1992;63(3):220-224.
- Jeng PY, Luzi AL, Pitarch RM, Chang MC, Wu YH, Jeng JH. Cemental tear: To know what we have neglected in dental practice. J Formos Med Assoc. 2018;117(4):261-267.
- Leknes KN, Lie T, Selvig KA. Cemental tear: a risk factor in periodontal attachment loss. J Periodontol. 1996;67(6):583-588.
- Watanabe C, Watanabe Y, Miyauchi M, Fujita M, Watanabe Y. Multiple cemental tears. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114(3):365-372.
- Pedercini A, Weitz D, Heyse Jr J, et al. Cemental tear: An overlooked finding associated with rapid periodontal destruction. A case series. Aust Dent J. 2021;66(S1):S82-S87.
- Tai TF, Chiang CP, Lin CP, Lin CC, Jeng JH. Persistent endodontic lesion due to complex cementodentinal tears in a maxillary central incisor—a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontology. 2007;103(6):e55-e60.
- Petti S, Glendor U, Andersson L. World traumatic dental injury prevalence and incidence, a meta-analysis-one billion living people have had traumatic dental injuries. Dent Traumatol. 2018;34(2):71-86.
- Lee AHC, Neelakantan P, Dummer PMH, Zhang C. Cemental tear: Literature review, proposed classification and recommendations for treatment. Int Endod J. 2021;54(11):2044-2073.
- Lin HJ, Chang SH, Chang MC, et al. Clinical fracture site, morphologic and histopathologic characteristics of cemental tear: role in endodontic lesions. J Endod. 2012;38(8):1058-1062.
- Damasceno LS, Dutra WO, Melgaço EG, Souza PEA de, Zenóbio EG, Horta MCR. Cemental tear: a case report with nonsurgical periodontal therapy. Rev Odonto Ciênc. 2012;27:74-77.
